Sections
Section I: Genotype Summary
Genotypes called: 6 / 18
| Drugs | Gene |
Genotypes
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CYP2B6 † ‡ |
Genotypes based on missing variant input *. |
||||||||||
|
|
CYP2C19 † ‡ |
Genotype based on missing variant input *. |
|||||||||
|
|
CYP2C9 † ‡ |
Genotypes based on missing variant input *. |
|||||||||
| DPYD † |
Genotypes based on missing variant input *. |
||||||||||
|
|
SLCO1B1 † ‡ |
Genotype based on missing variant input *. |
|||||||||
| TPMT † ‡ |
Genotype based on missing variant input *. |
Section II: Prescribing Recommendations
amitriptyline
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
Activity Scores
|
|
Initiate therapy with recommended starting dose.
Other ConsiderationsPatients may receive an initial low dose of a tricyclic, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose. |
Strong |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clinical pharmacology and therapeutics. 2013. PMID:23486447
- Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clinical pharmacology and therapeutics. 2017. PMID:27997040
atorvastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Function |
SLCO1B1: Typical myopathy risk and statin exposure |
Prescribe desired starting dose and adjust doses based on disease-specific guidelines.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong | |
|
DPWG Guideline Annotation 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
|
FDA PGx Association 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between SLCO1B1 and statins and CYP2C9 and sulfonylureas. European journal of human genetics : EJHG. 2024. PMID:39676086
- FDA Table of Pharmacogenetic Associations.
avatrombopag
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations." * | Unspecified |
Citations:
azathioprine
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotypes
|
|
Based on TPMT status, start with reduced starting doses (30%-80% of normal dose) if normal starting dose is 2-3 mg/kg/day (e.g., 0.6 – 2.4 mg/kg/day), and adjust doses of azathioprine based on degree of myelosuppression and disease-specific guidelines. Allow 2-4 weeks to reach steady-state after each dose adjustment (PMID 20354201, 11302950, 15606506, 16530532). NUDT15 genotype is not available. If thiopurines are required and NUDT15 status is unknown, monitor closely for toxicity.
Other ConsiderationsNormal starting doses vary by race/ethnicity and treatment regimens. If standard dose is below normal recommended dose, dose reduction might not be recommended for intermediate metabolizers. |
Strong |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
Grade ≥ 2 leukopaenia occurs in 23% of these patients with normal therapy for immunosuppression. The genetic variation increases the quantity of the active metabolites of azathioprine and mercaptopurine. | IMMUNOSUPPRESSION Start with 50% of the standard dose. Adjustment of the initial dose should be guided by toxicity (monitoring of blood counts) and effectiveness. Dose adjustment is not required for doses lower than 1.5 mg/kg per day for azathioprine or 0.75 mg/kg per day for mercaptopurine. Note: more stringent dose reductions are necessary if the patient is also NUDT15 IM or NUDT15 PM. | Unspecified |
|
Population: Dosing Info
|
Genotype
Phenotypes
|
"Consider...reduced dosages in patients with heterozygous [TPMT or NUDT15] deficiency...Because of the risk of increased toxicity, dosage reduction is recommended in patients known to have heterozygous deficiency of TPMT or NUDT15." See label for more information. * | Unspecified | |
|
Affected subgroup: TPMT and/or NUDT15 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotypes
|
"Alters systemic active metabolite concentration and dosage requirements. Results in higher adverse reaction risk (myelosuppression). Consider alternative therapy in poor metabolizers. Dosage reduction is recommended in intermediate metabolizers for NUDT15 or TPMT. Intermediate metabolizers for both genes may require more substantial dosage reductions. Refer to FDA labeling for specific dosing recommendations." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clinical pharmacology and therapeutics. 2011. PMID:21270794
- Clinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing: 2013 update. Clinical pharmacology and therapeutics. 2013. PMID:23422873
- Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clinical pharmacology and therapeutics. 2019. PMID:30447069
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA: Drug Product IMURAN (azathioprine), NDA016324, Sebela Pharmaceuticals Inc.
- FDA Table of Pharmacogenetic Associations.
brivaracetam
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
FDA Label Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C19 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations and higher adverse reaction risk. Consider dosage reductions in poor metabolizers." * | Unspecified | ||
capecitabine
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Metabolizer Activity Score
2.0 |
DPYD: Normal DPD activity and "normal" risk for fluoropyrimidine toxicity | Based on genotype, there is no indication to change dose or therapy. Use label-recommended dosage and administration. | Strong | |
|
Population: No Action
|
Genotype
Phenotype
2.0 (Normal Metabolizer) |
The guideline does not provide a description of the impact of a DPYD activity score of 2 on capecitabine. | The guideline does not provide a recommendation for capecitabine in patients with a DPYD activity score of 2. | No recommendation | |
|
FDA Label Annotation 1 |
Genotype
DPYD:c.85T>C (*9A);DPYD:c.496A>G |
|
|||
|
FDA PGx Association 1 |
Genotype
DPYD:c.85T>C (*9A);DPYD:c.496A>G |
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for dihydropyrimidine dehydrogenase genotype and fluoropyrimidine dosing. Clinical pharmacology and therapeutics. 2013. PMID:23988873
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clinical pharmacology and therapeutics. 2018. PMID:29152729
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction of DPYD and fluoropyrimidines. European journal of human genetics : EJHG. 2020. PMID:31745289
- Drugs@FDA: Drug Product Xeloda (capecitabine), NDA020896, Genentech, Inc.
- FDA Table of Pharmacogenetic Associations.
celecoxib
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Initiate therapy with lowest recommended starting dose. Titrate dose upward to clinical effect or maximum recommended dose with caution. In accordance with the prescribing information, use the lowest effective dosage for shortest duration consistent with individual patient treatment goals. Carefully monitor adverse events such as blood pressure and kidney function during course of therapy.
Other ConsiderationsIMs might have a higher than normal risk of adverse events especially in individuals with other factors affecting clearance of these drugs such as hepatic impairment or advanced age. Further caution should be taken with ibuprofen use in individuals carrying the CYP2C9*2 allele as it is in linkage disequilibrium with CYP2C8*3 and ibuprofen is also metabolized by CYP2C8. |
Moderate | |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation | |
|
FDA Label Annotation 1 |
Genotypes
CYP2C9:*1/*3;CYP2C9:*1/*18; CYP2C9:*1/*68 |
|
|||
|
Affected subgroup: CYP2C9 poor metabolizers or *3 carriers Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations. Reduce starting dose to half of the lowest recommended dose in poor metabolizers. Consider alternative therapy in poor metabolizers with juvenile rheumatoid arthritis." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
- Drugs@FDA: Drug Product CELEBREX (Celecoxib), NDA020998, Aphena Pharma Solutions - Tennessee, LLC.
- FDA Table of Pharmacogenetic Associations.
citalopram
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Reduced metabolism when compared to CYP2C19 normal metabolizers. Higher plasma concentrations may increase the probability of side effects. |
Initiate therapy with recommended starting dose. Consider a slower titration schedule and lower maintenance dose than normal metabolizers.
Other ConsiderationsDrug-drug interactions and other patient characteristics (e.g., age, renal function, liver function) should be considered when adjusting dose. |
Moderate | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
FDA Label Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
FDA PGx Association 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clinical pharmacology and therapeutics. 2015. PMID:25974703
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants. Clinical pharmacology and therapeutics. 2023. PMID:37032427
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2C19 and CYP2D6 and SSRIs. European journal of human genetics : EJHG. 2022. PMID:34782755
- Drugs@FDA: Drug Product Celexa (citalopram), NDA020822, Allergan, Inc.
- FDA Table of Pharmacogenetic Associations.
clobazam
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
FDA Label Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic active metabolite concentrations. Poor metabolism results in higher adverse reaction risk. Dosage adjustment is recommended. Refer to FDA labeling for specific dosing recommendations." * | Unspecified | ||
clomipramine
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
Activity Scores
|
|
Initiate therapy with recommended starting dose.
Other ConsiderationsPatients may receive an initial low dose of a tricyclic, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose. |
Optional | |
|
Genotypes
CYP2C19:*2/*38;CYP2D6:Not called - no variant data provided |
|
||||
Citations:
- Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clinical pharmacology and therapeutics. 2013. PMID:23486447
- Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clinical pharmacology and therapeutics. 2017. PMID:27997040
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
clopidogrel
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Alternate Drug
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Reduced clopidogrel active metabolite formation; increased on-treatment platelet reactivity; increased risk for adverse cardiac and cerebrovascular events |
Avoid standard dose (75 mg) clopidogrel if possible. Use prasugrel or ticagrelor at standard dose if no contraindication.
Other ConsiderationsFor cardiovascular indications of acute coronary syndrome (ACS) and/or percutaneous coronary intervention (PCI). ACS and/or PCI includes patients undergoing PCI for an ACS or non-ACS (elective) indication. |
Strong | |
|
Population: No Action
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Reduced clopidogrel active metabolite formation; increased on-treatment platelet reactivity; increased risk for adverse cardiac and cerebrovascular events |
No recommendation
Other ConsiderationsFor non-acute coronary syndrome (non-ACS) and non-percutaneous coronary intervention (non-PCI) cardiovascular indications. Non-ACS, non-PCI cardiovascular indications include peripheral arterial disease and stable coronary artery disease following a recent myocardial infarction outside the setting of PCI. |
No recommendation | |
|
Population: Alternate Drug
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Reduced clopidogrel active metabolite formation; increased on-treatment platelet reactivity; increased risk for adverse cardiac and cerebrovascular events |
Consider an alternative P2Y12 inhibitor at standard dose if clinically indicated and no contraindication.
Other ConsiderationsFor neurovascular indications. Neurovascular disease includes acute ischemic stroke or transient ischemic attack, secondary prevention of stroke, or prevention of thromboembolic events following neurointerventional procedures such as carotid artery stenting and stent-assisted coiling of intracranial aneurysms. Alternative P2Y12 inhibitors not impacted by CYP2C19 genetic variants include ticagrelor and ticlopidine. Prasugrel is contraindicated in patients with a history of stroke or TIA. Given limited outcomes data for genotype-guided anti-platelet therapy for neurovascular indications, selection of therapy should depend on individual patient treatment goals and risks for adverse events. |
Moderate | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
FDA Label Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C19 intermediate or poor metabolizers Alternate Drug
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in lower systemic active metabolite concentrations, lower antiplatelet response, and may result in higher cardiovascular risk. Consider use of another platelet P2Y12 inhibitor." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-2C19 (CYP2C19) genotype and clopidogrel therapy. Clinical pharmacology and therapeutics. 2011. PMID:21716271
- Clinical Pharmacogenetics Implementation Consortium guidelines for CYP2C19 genotype and clopidogrel therapy: 2013 update. Clinical pharmacology and therapeutics. 2013. PMID:23698643
- Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2C19 Genotype and Clopidogrel Therapy: 2022 Update. Clinical pharmacology and therapeutics. 2022. PMID:35034351
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA: Drug Product Plavix (clopidogrel bisulfate), NDA020839, Rebel Distributors Corp.
- Drugs@FDA: Drug Product Plavix (clopidogrel), sanofi-aventis U.S. LLC - NDA020839/SUPPL-78, 09/16/2022.
- FDA Table of Pharmacogenetic Associations.
dexlansoprazole
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Increased plasma concentration of PPI compared to CYP2C19 NMs; increased chance of efficacy and potentially toxicity | Initiate standard starting daily dose. For chronic therapy (>12 weeks) and efficacy achieved, consider 50% reduction in daily dose and monitor for continued efficacy. | Optional |
|
Affected subgroup: CYP2C19 intermediate or poor metabolizer Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clinical pharmacology and therapeutics. 2021. PMID:32770672
- FDA Table of Pharmacogenetic Associations.
doxepin
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
Activity Scores
|
|
Initiate therapy with recommended starting dose.
Other ConsiderationsPatients may receive an initial low dose of a tricyclic, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose. |
Optional |
|
Affected subgroup: CYP2C19 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clinical pharmacology and therapeutics. 2013. PMID:23486447
- Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clinical pharmacology and therapeutics. 2017. PMID:27997040
- FDA Table of Pharmacogenetic Associations.
dronabinol
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Monitoring for increased adverse reactions is recommended in patients known to carry genetic variants associated with diminished CYP2C9 function." See label for more information. * | Unspecified | |
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"May result in higher systemic concentrations and higher adverse reaction risk. Monitor for adverse reactions." * | Unspecified |
efavirenz
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Metabolizer |
CYP2B6: Normal efavirenz metabolism |
Initiate efavirenz with standard dosing (600 mg/day)
Other ConsiderationsThe ENCORE study showed that in treatment-naïve patients randomized to initiate efavirenz-based regimens (combined with tenofovir and emtricitabine), 400 mg/day was non-inferior to 600 mg/day regardless of CYP2B6 genotype (PMID 24522178). |
Strong | |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2B6: Higher dose-adjusted trough concentrations of efavirenz compared with normal metabolizers; increased risk of CNS adverse events |
Consider initiating efavirenz with decreased dose of 400 mg/day
Other ConsiderationsIf therapeutic drug monitoring is available and a decreased efavirenz dose is prescribed, consider obtaining steady-state plasma efavirenz concentrations to ensure concentrations are in the suggested therapeutic range (~1 to 4 μg/mL). To prescribe efavirenz at a decreased dose of 400 mg/day or 200 mg/day in a multidrug regimen may require prescribing more than one pill once daily. If so, the provider should weigh the potential benefit of reduced dose against the potential detrimental impact of increased pill number. |
Moderate | |
|
Population: No Action
|
Genotype
Phenotype
Normal Metabolizer |
The guideline does not provide a description of the impact of a normal metabolizer phenotype on efavirenz. | The guideline does not provide a recommendation for efavirenz in normal metabolizers. | No recommendation | |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
Genetic variations increase the efavirenz plasma concentration and therefore the risk of side effects. However, the efavirenz plasma concentration remains within the therapeutic range for the majority of patients. | Determine the efavirenz plasma concentration if side effects occur and reduce the dose if needed. In 14 IM adults, a dose reduction to 400 mg/day (2/3rd of the standard dose) was sufficient to achieve therapeutic plasma concentrations and to reduce or resolve side effects. The therapeutic range established for efavirenz is 1000-4000 ng/ml. | Unspecified | |
|
FDA PGx Association 1 |
Genotypes
CYP2B6:*1/*5;CYP2B6:*1/*7 |
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2B6 and Efavirenz-Containing Antiretroviral Therapy. Clinical pharmacology and therapeutics. 2019. PMID:31006110
- FDA Table of Pharmacogenetic Associations.
escitalopram
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Reduced metabolism when compared to CYP2C19 normal metabolizers. Higher plasma concentrations may increase the probability of side effects. |
Initiate therapy with recommended starting dose. Consider a slower titration schedule and lower maintenance dose than normal metabolizers.
Other ConsiderationsDrug-drug interactions and other patient characteristics (e.g., age, renal function, liver function) should be considered when adjusting dose. |
Moderate | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C19 ultrarapid, intermediate, or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"May alter systemic concentrations." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clinical pharmacology and therapeutics. 2015. PMID:25974703
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants. Clinical pharmacology and therapeutics. 2023. PMID:37032427
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2C19 and CYP2D6 and SSRIs. European journal of human genetics : EJHG. 2022. PMID:34782755
- FDA Table of Pharmacogenetic Associations.
flucytosine
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
2.0 (Normal Metabolizer) |
The guideline does not provide a description of the impact of a DPYD activity score of 2 on flucytosine. | The guideline does not provide a recommendation for flucytosine in patients with a DPYD activity score of 2. | No recommendation |
fluorouracil
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Metabolizer Activity Score
2.0 |
DPYD: Normal DPD activity and "normal" risk for fluoropyrimidine toxicity | Based on genotype, there is no indication to change dose or therapy. Use label-recommended dosage and administration. | Strong | |
|
Population: No Action
|
Genotype
Phenotype
2.0 (Normal Metabolizer) |
The guideline does not provide a description of the impact of a DPYD activity score of 2 on fluorouracil. | The guideline does not provide a recommendation for fluorouracil in patients with a DPYD activity score of 2. | No recommendation | |
|
FDA Label Annotation 1 |
Genotype
DPYD:c.85T>C (*9A);DPYD:c.496A>G |
|
|||
|
FDA PGx Association 1 |
Genotype
DPYD:c.85T>C (*9A);DPYD:c.496A>G |
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for dihydropyrimidine dehydrogenase genotype and fluoropyrimidine dosing. Clinical pharmacology and therapeutics. 2013. PMID:23988873
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing: 2017 Update. Clinical pharmacology and therapeutics. 2018. PMID:29152729
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction of DPYD and fluoropyrimidines. European journal of human genetics : EJHG. 2020. PMID:31745289
- Drugs@FDA: Drug Product Carac (fluorouracil), Bausch Health US, LLC - NDA020985/SUPPL-19, 05/26/2022.
- Drugs@FDA: Drug Product FLUOROURACIL (FLUOROURACIL), Eugia US LLC - ANDA202669/SUPPL-9, 03/21/2024.
- Drugs@FDA: Drug Product Fluorouracil (Fluorouracil), BluePoint Laboratories - ANDA210124/SUPPL-9, 03/21/2024.
- FDA Table of Pharmacogenetic Associations.
flurbiprofen
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Initiate therapy with lowest recommended starting dose. Titrate dose upward to clinical effect or maximum recommended dose with caution. In accordance with the prescribing information, use the lowest effective dosage for shortest duration consistent with individual patient treatment goals. Carefully monitor adverse events such as blood pressure and kidney function during course of therapy.
Other ConsiderationsIMs might have a higher than normal risk of adverse events especially in individuals with other factors affecting clearance of these drugs such as hepatic impairment or advanced age. Further caution should be taken with ibuprofen use in individuals carrying the CYP2C9*2 allele as it is in linkage disequilibrium with CYP2C8*3 and ibuprofen is also metabolized by CYP2C8. |
Moderate | |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation | |
|
FDA Label Annotation 1 |
Genotypes
CYP2C9:*1/*3;CYP2C9:*1/*18; CYP2C9:*1/*68 |
|
|||
|
Affected subgroup: CYP2C9 poor metabolizers or *3 carriers Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations. Use a reduced dosage in poor metabolizers." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
- Drugs@FDA: Drug Product FLURBIPROFEN SODIUM (flurbiprofen sodium), NDA019404, Rebel Distributors Corp.
- Drugs@FDA: Drug Product flurbiprofen (NDA018766)
- FDA Table of Pharmacogenetic Associations.
fluvastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Alternate Drug
Dosing Info
|
Genotype
Phenotypes
Activity Scores
|
|
Prescribe ≤40mg per day as a starting dose and adjust doses of fluvastatin based on disease-specific guidelines. If dose >40mg needed for desired efficacy, consider an alternative statin or combination therapy (i.e., fluvastatin plus non-statin guideline directed medical therapy) (PMID: 30423391).
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function should be evaluated prior to initiating a statin. The effects of drug-drug interactions may be more pronounced resulting in a higher risk of myopathy. |
Moderate |
|
Population: No Action
|
Genotypes
Phenotypes
Activity Scores
|
|
Based on SLCO1B1 status, prescribe desired starting dose and adjust doses based on disease-specific guidelines. CYP2C9 phenotype could not be assigned based on genotyping.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong |
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
fosphenytoin
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
|
For first dose, use typical initial or loading dose. For subsequent doses, use approximately 25% less than typical maintenance dose. Subsequent doses should be adjusted according to therapeutic drug monitoring, response and side effects. An HLA-B*15:02 negative test does not eliminate the risk of phenytoin-induced SJS/TEN, and patients should be carefully monitored according to a usual standard. | Moderate |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
|
For first dose, use typical initial or loading dose. For subsequent doses, use approximately 25% less than typical maintenance dose. Subsequent doses should be adjusted according to therapeutic drug monitoring, response and side effects. An HLA-B*15:02 negative test does not eliminate the risk of phenytoin-induced SJS/TEN, and patients should be carefully monitored according to a usual standard. | Moderate |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Scores
|
|
No recommendation | Unspecified |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Scores
|
|
No recommendation | Unspecified |
|
Population: Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
"Consider avoiding CEREBYX [fosphenytoin] as an alternative to carbamazepine in patients who are positive for HLA-B*1502 or in CYP2C9*3 carriers. Should CEREBYX [fosphenytoin] be utilized for CYP2C9*3 carriers, consider starting at the lower end of the dosage range...[P]atients who are known to be intermediate or poor metabolizers may ultimately require lower doses to maintain similar steady-state concentrations compared to normal metabolizers. In patients who are known to be carriers of the decreased function CYP2C9*2 or *3 alleles (intermediate and poor metabolizers), consider starting at the low end of the dosage range and monitor serum concentrations to maintain total phenytoin concentrations of 10 to 20 mcg/mL." See label for more information. * | Unspecified | |
|
CYP2C9 intermediate or poor metabolizers Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"May result in higher systemic concentrations and higher adverse reaction risk (central nervous system toxicity). Consider starting at the lower end of the dosage range and monitor serum concentrations. Refer to FDA labeling for specific dosing recommendations. Carriers of CYP2C9*3 alleles may be at increased risk of severe cutaneous adverse reactions. Consider avoiding fosphenytoin as an alternative to carbamazepine in patients who are CYP2C9*3 carriers. Genotyping is not a substitute for clinical vigilance and patient management." * | Unspecified |
Citations:
- Clinical pharmacogenetics implementation consortium guidelines for CYP2C9 and HLA-B genotypes and phenytoin dosing. Clinical pharmacology and therapeutics. 2014. PMID:25099164
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C9 and HLA-B Genotypes and Phenytoin Dosing: 2020 Update. Clinical pharmacology and therapeutics. 2021. PMID:32779747
- Drugs@FDA: Drug Product CEREBYX (Fosphenytoin Sodium), NDA020450, Pfizer Laboratories Div Pfizer Inc.
- FDA Table of Pharmacogenetic Associations.
ibuprofen
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Initiate therapy with lowest recommended starting dose. Titrate dose upward to clinical effect or maximum recommended dose with caution. In accordance with the prescribing information, use the lowest effective dosage for shortest duration consistent with individual patient treatment goals. Carefully monitor adverse events such as blood pressure and kidney function during course of therapy.
Other ConsiderationsIMs might have a higher than normal risk of adverse events especially in individuals with other factors affecting clearance of these drugs such as hepatic impairment or advanced age. Further caution should be taken with ibuprofen use in individuals carrying the CYP2C9*2 allele as it is in linkage disequilibrium with CYP2C8*3 and ibuprofen is also metabolized by CYP2C8. |
Moderate | |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation | |
|
FDA PGx Association 1 |
Genotypes
CYP2C9:*1/*3;CYP2C9:*1/*18; CYP2C9:*1/*68 |
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
- FDA Table of Pharmacogenetic Associations.
imipramine
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
Activity Scores
|
|
Initiate therapy with recommended starting dose.
Other ConsiderationsPatients may receive an initial low dose of a tricyclic, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose. |
Optional | |
|
Genotypes
CYP2C19:*2/*38;CYP2D6:Not called - no variant data provided |
|
||||
Citations:
- Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clinical pharmacology and therapeutics. 2013. PMID:23486447
- Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clinical pharmacology and therapeutics. 2017. PMID:27997040
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
lansoprazole
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Increased plasma concentration of PPI compared to CYP2C19 NMs; increased chance of efficacy and potentially toxicity | Initiate standard starting daily dose. For chronic therapy (>12 weeks) and efficacy achieved, consider 50% reduction in daily dose and monitor for continued efficacy. | Optional | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
FDA PGx Association 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clinical pharmacology and therapeutics. 2021. PMID:32770672
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- FDA Table of Pharmacogenetic Associations.
lornoxicam
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Initiate therapy with lowest recommended starting dose. Titrate dose upward to clinical effect or maximum recommended dose with caution. In accordance with the prescribing information, use the lowest effective dosage for shortest duration consistent with individual patient treatment goals. Carefully monitor adverse events such as blood pressure and kidney function during course of therapy.
Other ConsiderationsIMs might have a higher than normal risk of adverse events especially in individuals with other factors affecting clearance of these drugs such as hepatic impairment or advanced age. Further caution should be taken with ibuprofen use in individuals carrying the CYP2C9*2 allele as it is in linkage disequilibrium with CYP2C8*3 and ibuprofen is also metabolized by CYP2C8. |
Moderate |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation |
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
lovastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Function |
SLCO1B1: Typical myopathy risk and statin exposure |
Prescribe desired starting dose and adjust doses based on disease-specific guidelines.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong |
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
mavacamten
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations and may have higher adverse reaction risk (heart failure). Dosage is based on individual response. The dose titration and monitoring schedule accounts for differences due to CYP2C19 genetic variation, so adjustments based on CYP2C19 genotype are not necessary. Refer to FDA labeling for specific dosing recommendations and monitoring." * | Unspecified |
Citations:
meloxicam
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Initiate therapy with 50% of the lowest recommended starting dose. Titrate dose upward to clinical effect or 50% of the maximum recommended dose with caution. In accordance with the meloxicam prescribing information, use the lowest effective dosage for shortest duration consistent with individual patient treatment goals. Upward dose titration should not occur until after steady state is reached (at least 7 days). Carefully monitor adverse events such as blood pressure and kidney function during course of therapy. Alternatively, consider alternative therapy. Choose an alternative therapy not metabolized by CYP2C9 or not significantly impacted by CYP2C9 genetic variants in vivo or choose an NSAID metabolized by CYP2C9 but with a shorter half-life (see CPIC THERAPEUTIC RECOMMENDATIONS FOR CELECOXIB, FLURBIPROFEN, LORNOXICAM, AND IBUPROFEN BASED ON CYP2C9 PHENOTYPE).
Other ConsiderationsIMs might have a higher than normal risk of adverse events especially in individuals with other factors affecting clearance of these drugs such as hepatic impairment or advanced age. Alternative therapies not primarily metabolized by CYP2C9 include aspirin, ketorolac, naproxen and sulindac. Selection of therapy will depend on individual patient treatment goals and risks for toxicity. |
Moderate |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation |
|
Affected subgroup: CYP2C9 poor metabolizers or *3 carriers Dosing Info
Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations. Consider dose reductions in poor metabolizers. Monitor patients for adverse reactions." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
- FDA Table of Pharmacogenetic Associations.
mercaptopurine
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotypes
|
|
Based on TPMT status, start with reduced starting doses (30%-80% of normal dose) if normal starting dose is ≥ 75 mg/m2/day or ≥ 1.5 mg/kg/day (e.g., start at 22.5-60 mg/m2/day or 0.45-1.2 mg/kg/day) and adjust doses of mercaptopurine based on degree of myelosuppression and disease-specific guidelines. Allow 2-4 weeks to reach steady-state after each dose adjustment. If myelosuppression occurs, and depending on other therapy, emphasis should be on reducing mercaptopurine over other agents (PMID 20354201,18685564, 8857546, 18987654, 20010622, 16401827, 11302950, 16530532, 9634537). If normal starting dose is already < 75 mg/m2/day or < 1.5 mg/kg/day, dose reduction may not be recommended. NUDT15 genotype result is not available. If thiopurines are required and either TPMT or NUDT15 status is unknown, monitor closely for toxicity.
Other ConsiderationsNormal starting doses vary by race/ethnicity and treatment regimens. If standard dose is below normal recommended dose, dose reduction might not be recommended for intermediate metabolizers. |
Strong |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
Grade ≥ 2 leukopaenia occurs in 23% of these patients with normal therapy for immunosuppression. The genetic variation increases the quantity of the active metabolites of azathioprine and mercaptopurine | IMMUNOSUPPRESSION: Start with 50% of the standard dose. Adjustment of the initial dose should be guided by toxicity (monitoring of blood counts) and effectiveness. Dose adjustment is not required for doses lower than 1.5 mg/kg per day for azathioprine or 0.75 mg/kg per day for mercaptopurine. LEUKAEMIA: Start with 50% of the standard mercaptopurine dose, or start with the standard dose and reduce to 50% if side effects necessitate a dose reduction. It is not known whether dose reduction in advance results in the same efficacy as dose reduction based on toxicity. The initial dose should be adjusted based on toxicity (monitoring of the blood counts) and efficacy. Note: more stringent dose reductions are necessary if the patient is also NUDT15 IM or NUDT15 PM. | Unspecified |
|
Population: Dosing Info
|
Genotype
Phenotypes
|
The mercaptopurine (PURIXAN) label states: "Heterozygous Deficiency in TPMT and/or NUDT15 … Reduce the PURIXAN dosage based on tolerability. Most patients with heterozygous TPMT or NUDT15 deficiency tolerate recommended dosage, but some require dose reduction based on adverse reactions. Patients who are heterozygous for both TPMT and NUDT15 may require more substantial dose reductions.” See label for more information. * | Unspecified | |
|
Affected subgroup: TPMT and/or NUDT15 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotypes
|
"Alters systemic active metabolite concentration and dosage requirements. Results in higher adverse reaction risk (myelosuppression). Initial dosages should be reduced in poor metabolizers; poor metabolizers generally tolerate 10% or less of the recommended dosage. Intermediate metabolizers may require dosage reductions based on tolerability. Intermediate metabolizers for both genes may require more substantial dosage reductions. Refer to FDA labeling for specific dosing recommendations." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clinical pharmacology and therapeutics. 2011. PMID:21270794
- Clinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing: 2013 update. Clinical pharmacology and therapeutics. 2013. PMID:23422873
- Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clinical pharmacology and therapeutics. 2019. PMID:30447069
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA: Drug Product PURINETHOL (Mercaptopurine), Quinn Pharmaceuticals - NDA009053/SUPPL-40, 12/29/2020.
- Drugs@FDA: Drug Product PURIXAN (mercaptopurine), Nova Laboratories, Ltd - NDA205919/SUPPL-4, 04/07/2020.
- FDA Table of Pharmacogenetic Associations.
omeprazole
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Increased plasma concentration of PPI compared to CYP2C19 NMs; increased chance of efficacy and potentially toxicity | Initiate standard starting daily dose. For chronic therapy (>12 weeks) and efficacy achieved, consider 50% reduction in daily dose and monitor for continued efficacy. | Optional | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C19 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clinical pharmacology and therapeutics. 2021. PMID:32770672
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- FDA Table of Pharmacogenetic Associations.
pantoprazole
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Increased plasma concentration of PPI compared to CYP2C19 NMs; increased chance of efficacy and potentially toxicity | Initiate standard starting daily dose. For chronic therapy (>12 weeks) and efficacy achieved, consider 50% reduction in daily dose and monitor for continued efficacy. | Optional | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
FDA Label Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Pediatrics; Affected subgroup: CYP2C19 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations. Consider dosage reduction in children who are poor metabolizers. No dosage adjustment is needed for adult patients who are intermediate or poor metabolizers." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clinical pharmacology and therapeutics. 2021. PMID:32770672
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA: Drug Product Protonix Delayed-Release (PANTOPRAZOLE SODIUM), NDA020987, Avera McKennan Hospital.
- FDA Table of Pharmacogenetic Associations.
phenytoin
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
|
For first dose, use typical initial or loading dose. For subsequent doses, use approximately 25% less than typical maintenance dose. Subsequent doses should be adjusted according to therapeutic drug monitoring, response and side effects. An HLA-B*15:02 negative test does not eliminate the risk of phenytoin-induced SJS/TEN, and patients should be carefully monitored according to a usual standard. | Moderate |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
|
For first dose, use typical initial or loading dose. For subsequent doses, use approximately 25% less than typical maintenance dose. Subsequent doses should be adjusted according to therapeutic drug monitoring, response and side effects. An HLA-B*15:02 negative test does not eliminate the risk of phenytoin-induced SJS/TEN, and patients should be carefully monitored according to a usual standard. | Moderate |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Scores
|
|
No recommendation | Unspecified |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Scores
|
|
No recommendation | Unspecified |
|
Population: Dosing Info
Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
Genetic variation reduces conversion of phenytoin to inactive metabolites. This increases the risk of side effects. The life-threatening cutaneous side effects Stevens-Johnson Syndrome and toxic epidermal necrolysis may occur, especially in Asian patients. |
|
Unspecified |
|
Population: Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Scores
|
"Patients who are intermediate or poor metabolizers of CYP2C9 substrates (e.g., *1/*3, *2/*2, *3/*3) may exhibit increased phenytoin serum concentrations compared to patients who are normal metabolizers (e.g., *1/*1). Thus, patients who are known to be intermediate or poor metabolizers may ultimately require lower doses of phenytoin to maintain similar steady-state concentrations compared to normal metabolizers...Consider avoiding DILANTIN [phenytoin] as an alternative to carbamazepine in patients who are positive for HLA-B*1502 or in CYP2C9*3 carriers." See label for more information. * | Unspecified | |
|
CYP2C9 intermediate or poor metabolizers Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"May result in higher systemic concentrations and higher adverse reaction risk (central nervous system toxicity). Refer to FDA labeling for specific dosing recommendations. Carriers of CYP2C9*3 alleles may be at increased risk of severe cutaneous adverse reactions. Consider avoiding phenytoin as an alternative to carbamazepine in patients who are CYP2C9*3 carriers. Genotyping is not a substitute for clinical vigilance and patient management." * | Unspecified |
Citations:
- Clinical pharmacogenetics implementation consortium guidelines for CYP2C9 and HLA-B genotypes and phenytoin dosing. Clinical pharmacology and therapeutics. 2014. PMID:25099164
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C9 and HLA-B Genotypes and Phenytoin Dosing: 2020 Update. Clinical pharmacology and therapeutics. 2021. PMID:32779747
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA Drug Product: DILANTIN (phenytoin), NDA008762, Upjohn.
- FDA Table of Pharmacogenetic Associations.
piroxicam
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Alternate Drug
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Choose an alternative therapy not metabolized by CYP2C9 or not significantly impacted by CYP2C9 genetic variants in vivo or choose an NSAID metabolized by CYP2C9 but with a shorter half-life (see CPIC THERAPEUTIC RECOMMENDATIONS FOR CELECOXIB, FLURBIPROFEN, LORNOXICAM, AND IBUPROFEN BASED ON CYP2C9 PHENOTYPE).
Other ConsiderationsAlternative therapies not primarily metabolized by CYP2C9 include aspirin, ketorolac, naproxen and sulindac. Selection of therapy will depend on individual patient treatment goals and risks for toxicity. |
Moderate | |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation | |
|
FDA Label Annotation 1 |
Genotypes
CYP2C9:*1/*3;CYP2C9:*1/*18; CYP2C9:*1/*68 |
|
|||
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations. Consider reducing dosage in poor metabolizers." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
- Drugs@FDA: Drug Product Feldene (piroxicam), NDA018147, Pfizer Laboratories Div Pfizer Inc.
- FDA Table of Pharmacogenetic Associations.
pitavastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Function |
SLCO1B1: Typical myopathy risk and statin exposure |
Prescribe desired starting dose and adjust doses based on disease-specific guidelines.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong |
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
pravastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Function |
SLCO1B1: Typical myopathy risk and statin exposure |
Prescribe desired starting dose and adjust doses based on disease-specific guidelines.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong |
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
rosuvastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
|
|
Based on SLCO1B1 status, prescribe desired starting dose and adjust doses based on disease-specific guidelines. ABCG2 genotype result is not available.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong | |
|
DPWG Guideline Annotation 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
|
FDA PGx Association 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
Citations:
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between SLCO1B1 and statins and CYP2C9 and sulfonylureas. European journal of human genetics : EJHG. 2024. PMID:39676086
- FDA Table of Pharmacogenetic Associations.
sertraline
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotypes
|
|
Initiate therapy with recommended starting dose. Consider a slower titration schedule and lower maintenance dose. | Moderate | |
|
Population: Dosing Info
|
Genotype
Phenotypes
|
|
Initiate therapy with recommended starting dose. Consider a slower titration schedule and lower maintenance dose than normal metabolizers. | Optional | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clinical pharmacology and therapeutics. 2015. PMID:25974703
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants. Clinical pharmacology and therapeutics. 2023. PMID:37032427
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2C19 and CYP2D6 and SSRIs. European journal of human genetics : EJHG. 2022. PMID:34782755
simvastatin
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Normal Function |
SLCO1B1: Typical myopathy risk and statin exposure |
Prescribe desired starting dose and adjust doses based on disease-specific guidelines.
Other ConsiderationsThe potential for drug-drug interactions and dose limits based on renal and hepatic function and ancestry should be evaluated prior to initiating a statin. |
Strong | |
|
DPWG Guideline Annotation 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
|
FDA PGx Association 1 |
Genotype
SLCO1B1:*1/*20
|
|
|||
Citations:
- The clinical pharmacogenomics implementation consortium: CPIC guideline for SLCO1B1 and simvastatin-induced myopathy. Clinical pharmacology and therapeutics. 2012. PMID:22617227
- The clinical pharmacogenetics implementation consortium guideline for SLCO1B1 and simvastatin-induced myopathy: 2014 update. Clinical pharmacology and therapeutics. 2014. PMID:24918167
- The Clinical Pharmacogenetics Implementation Consortium Guideline for SLCO1B1, ABCG2, and CYP2C9 genotypes and Statin-Associated Musculoskeletal Symptoms. Clinical pharmacology and therapeutics. 2022. PMID:35152405
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between SLCO1B1 and statins and CYP2C9 and sulfonylureas. European journal of human genetics : EJHG. 2024. PMID:39676086
- FDA Table of Pharmacogenetic Associations.
siponimod
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
Theoretically, the risk of adverse effects in increased, as the genetic variation results in higher plasma concentrations of siponimod. | Use 50% of the normal maintenance dose. Reconsider the choice and the potential benefit of siponimod if the patient is also using a moderate CYP3A4 inducer, such as modafinil. For this genetic variation, a moderate CYP3A4 inducer results in a reduction in the exposure of siponimod by 49%, according to a pharmacokinetic model. | Unspecified |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
The MAYZENT (siponimod) label states: "Initiate MAYZENT with a 4-day titration, as shown in Table 2... Do not use the starter pack for patients who will be titrated to the 1-mg maintenance dosage." "In patients with a CYP2C9 *1/*3 or *2/*3 genotype, after treatment titration (see Treatment Initiation), the recommended maintenance dosage of MAYZENT is 1 mg taken orally once daily starting on Day 5." See label for more information. * | Unspecified | |
|
Affected subgroup: CYP2C9 intermediate or poor metabolizers Alternate Drug
Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Results in higher systemic concentrations. Adjust dosage based on genotype. Do not use in patients with CYP2C9 *3/*3 genotype. Refer to FDA labeling for specific dosing recommendations." * | Unspecified |
tegafur
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
2.0 (Normal Metabolizer) |
The guideline does not provide a description of the impact of a DPYD activity score of 2 on tegafur. | The guideline does not provide a recommendation for tegafur in patients with a DPYD activity score of 2. | No recommendation |
Citations:
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction of DPYD and fluoropyrimidines. European journal of human genetics : EJHG. 2020. PMID:31745289
tenoxicam
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Alternate Drug
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
CYP2C9: Moderately reduced metabolism; higher plasma concentrations may increase probability of toxicities |
Choose an alternative therapy not metabolized by CYP2C9 or not significantly impacted by CYP2C9 genetic variants in vivo or choose an NSAID metabolized by CYP2C9 but with a shorter half-life (see CPIC THERAPEUTIC RECOMMENDATIONS FOR CELECOXIB, FLURBIPROFEN, LORNOXICAM, AND IBUPROFEN BASED ON CYP2C9 PHENOTYPE).
Other ConsiderationsAlternative therapies not primarily metabolized by CYP2C9 include aspirin, ketorolac, naproxen and sulindac. Selection of therapy will depend on individual patient treatment goals and risks for toxicity. |
Optional |
|
Population: No Action
|
Genotypes
Phenotype
Indeterminate Activity Score
N/A |
CYP2C9: n/a | No recommendation | No recommendation |
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guideline (CPIC) for CYP2C9 and Nonsteroidal Anti-Inflammatory Drugs. Clinical pharmacology and therapeutics. 2020. PMID:32189324
thioguanine
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: Dosing Info
|
Genotype
Phenotypes
|
|
Based on TPMT status, start with reduced doses (50% to 80% of normal dose) if normal starting dose is ≥ 40-60 mg/m2/day (e.g., 20-48 mg/m2/day) and adjust doses of thioguanine based on degree of myelosuppression and disease-specific guidelines. Allow 2-4 weeks to reach steady-state after each dose adjustment. If myelosuppression occurs, and depending on other therapy, emphasis should be on reducing thioguanine over other agents (PMID 20354201, 11037857). NUDT15 genotype is not available. If thiopurines are required and NUDT15 status is unknown, monitor closely for toxicity.
Other ConsiderationsNormal starting doses vary by race/ethnicity and treatment regimens. If standard dose is below normal recommended dose, dose reduction might not be recommended for intermediate metabolizers. |
Moderate |
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
Genetic variation reduces conversion of thioguanine to inactive metabolites. This increases the risk of serious adverse events such as myelosuppression. | IMMUNOSUPPRESSION: Start with 75% of the standard dose. Adjustment of the initial dose should be guided by toxicity (monitoring of blood counts) and efficacy. The frequency of monitoring should be increased. LEUKAEMIA: Start with 75% of the standard thioguanine dose, or start with the standard dose and reduce to 75% if side effects necessitate a dose reduction. It is not known whether dose reduction in advance results in the same efficacy as dose reduction based on toxicity. The initial dose should be adjusted based on toxicity (monitoring of the blood counts) and efficacy. Monitoring should be performed at an increased frequency. Note: more stringent dose reductions are necessary if the patient is also NUDT15 IM. | Unspecified |
|
Population: Dosing Info
|
Genotype
Phenotypes
|
"Most patients with heterozygous TPMT or NUDT15 deficiency tolerate recommended thioguanine doses, but some require dose reduction based on toxicities...Reduce the dosage based on tolerability." See label for more information. * | Unspecified | |
|
Affected subgroup: TPMT and/or NUDT15 intermediate or poor metabolizers Dosing Info
|
Genotype
Phenotypes
|
"Alters systemic active metabolite concentration and dosage requirements. Results in higher adverse reaction risk (myelosuppression). Initial dosages should be reduced in poor metabolizers; poor metabolizers generally tolerate 10% or less of the recommended dosage. Intermediate metabolizers may require dosage reductions based on tolerability. Intermediate metabolizers for both genes may require more substantial dosage reductions. Refer to FDA labeling for specific dosing recommendations." * | Unspecified |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing. Clinical pharmacology and therapeutics. 2011. PMID:21270794
- Clinical pharmacogenetics implementation consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosing: 2013 update. Clinical pharmacology and therapeutics. 2013. PMID:23422873
- Clinical Pharmacogenetics Implementation Consortium Guideline for Thiopurine Dosing Based on TPMT and NUDT15 Genotypes: 2018 Update. Clinical pharmacology and therapeutics. 2019. PMID:30447069
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- Drugs@FDA: Drug Product TABLOID (thioguanine), NDA012429, Aspen Global Inc.
- FDA Table of Pharmacogenetic Associations.
trimipramine
| Source | Genes | Implications | Recommendation | Classification |
|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotypes
Activity Scores
|
|
Initiate therapy with recommended starting dose.
Other ConsiderationsPatients may receive an initial low dose of a tricyclic, which is then increased over several days to the recommended steady-state dose. The starting dose in this guideline refers to the recommended steady-state dose. |
Optional |
Citations:
- Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. Clinical pharmacology and therapeutics. 2013. PMID:23486447
- Clinical pharmacogenetics implementation consortium guideline (CPIC) for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants: 2016 update. Clinical pharmacology and therapeutics. 2017. PMID:27997040
voriconazole
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: No Action
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Higher dose-adjusted trough concentrations of voriconazole compared with normal metabolizers |
Initiate therapy with recommended standard of care dosing
Other ConsiderationsFurther dose adjustments or selection of alternative therapy may be necessary due to other clinical factors, such as drug interactions, hepatic function, renal function, species, site of infection, therapeutic drug monitoring, and comorbidities. |
Moderate | |
|
Population: No Action
|
Genotype
Phenotype
Intermediate Metabolizer |
CYP2C19: Higher dose-adjusted trough concentrations of voriconazole compared with normal metabolizers |
Initiate therapy with recommended standard of care dosing
Other ConsiderationsFurther dose adjustments or selection of alternative therapy may be necessary due to other clinical factors, such as drug interactions, hepatic function, renal function, species, site of infection, therapeutic drug monitoring, and comorbidities. |
Moderate | |
|
DPWG Guideline Annotation 1 |
Genotype
CYP2C19:*2/*38
|
|
|||
|
Affected subgroup: CYP2C19 intermediate or poor metabolizers Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer |
"Results in higher systemic concentrations and may result in higher adverse reaction risk." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for CYP2C19 and Voriconazole Therapy. Clinical pharmacology and therapeutics. 2017. PMID:27981572
- Pharmacogenetics: from bench to byte--an update of guidelines. Clinical pharmacology and therapeutics. 2011. PMID:21412232
- FDA Table of Pharmacogenetic Associations.
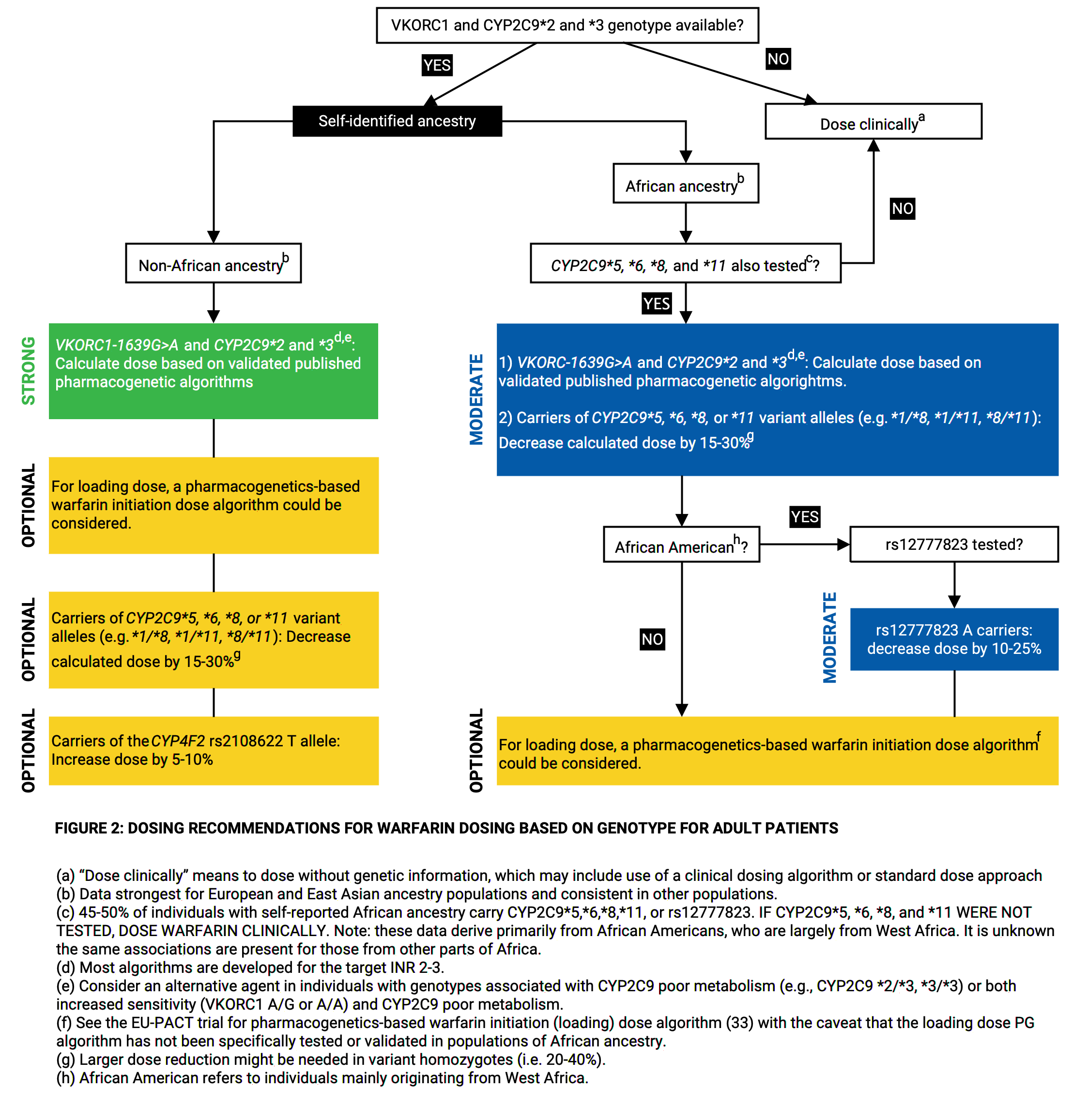
warfarin
| Source | Genes | Implications | Recommendation | Classification | |
|---|---|---|---|---|---|
|
Population: |
Genotypes
|
|
|||
|
Population: Dosing Info
|
Genotype
Phenotype
Intermediate Metabolizer |
This gene variation reduces the conversion of warfarin to inactive metabolites. This can increase the risk of bleeding. |
|
Unspecified | |
|
FDA Label Annotation 1 |
Genotypes
CYP2C9:*1/*3;CYP2C9:*1/*18; CYP2C9:*1/*68; VKORC1:Not called - no variant data provided |
|
|||
|
CYP2C9 intermediate or poor metabolizers Dosing Info
Other Guidance
|
Genotype
Phenotype
Intermediate Metabolizer Activity Score
1.0 |
"Alters systemic concentrations and dosage requirements. Select initial dosage, taking into account clinical and genetic factors. Monitor and adjust dosages based on INR." * | Unspecified | ||
Citations:
- Clinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C9 and VKORC1 genotypes and warfarin dosing. Clinical pharmacology and therapeutics. 2011. PMID:21900891
- Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for Pharmacogenetics-Guided Warfarin Dosing: 2017 Update. Clinical pharmacology and therapeutics. 2017. PMID:28198005
- Drugs@FDA: Drug Product COUMADIN (warfarin sodium), NDA009218, Bristol-Myers Squibb Pharma Company.
- FDA Table of Pharmacogenetic Associations.
Section III: Allele Matching Details
- CYP2B6 allele match data
- CYP2C19 allele match data
- CYP2C9 allele match data
- DPYD allele match data
- SLCO1B1 allele match data
- TPMT allele match data
No data provided for ABCG2, CACNA1S, CFTR, CYP2D6, CYP3A4, CYP3A5, CYP4F2, G6PD, NUDT15, RYR1, UGT1A1, VKORC1.
CYP2B6 allele match data
| Alleles Matched: |
|
|---|---|
| Phasing Status: |
Unphased It reports the genotype(s) that receive the highest score during the matcher process. In case of unphased data, additional genotypes might be possible and cannot be ruled out. |
| Alleles Not Considered: |
The following alleles are not considered due to 46 missing positions of the total 47 positions: *2, *3, *4, *6, *8, *9, *10, *11, *12, *13, *14, *15, *17, *18, *19, *20, *21, *22, *23, *24, *25, *26, *27, *28, *31, *32, *35, *36, *37, *38, *39, *40, *41, *42, *43, *44, *45, *46, *47, *48, *49 Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr19:41016810 | rs3211371 | C/T | C |
|
|
| chr19:40991224 | rs34223104 | Missing |
T |
|
|
| chr19:40991367 | rs34883432 | Missing |
A |
|
|
| chr19:40991369 | rs8192709 | Missing |
C |
|
|
| chr19:40991381 | rs33973337 | Missing |
A |
|
|
| chr19:40991388 | rs33980385 | Missing |
A |
|
|
| chr19:40991390 | rs33926104 | Missing |
C |
|
|
| chr19:40991391 | rs34284776 | Missing |
G |
|
|
| chr19:40991441 | rs35303484 | Missing |
A |
|
|
| chr19:41004015 | rs281864907 | Missing |
T |
|
|
| chr19:41004125 | rs36060847 | Missing |
G |
|
|
| chr19:41004133 | rs148009906 | Missing |
G |
|
|
| chr19:41004158 | rs186335453 | Missing |
G |
|
|
| chr19:41004303 | rs139801276 | Missing |
T |
|
|
| chr19:41004377 | rs12721655 | Missing |
A |
|
|
| chr19:41004380 | rs535039125 | Missing |
C |
|
|
| chr19:41004381 | rs35773040 | Missing |
G |
|
|
| chr19:41004406 | rs145884402 | Missing |
G |
|
|
| chr19:41006919 | rs3826711 | Missing |
C |
|
|
| chr19:41006923 | rs36056539 | Missing |
C |
|
|
| chr19:41006936 | rs3745274 | Missing |
G |
|
|
| chr19:41006967 | rs58871670 | Missing |
G |
|
|
| chr19:41006968 | rs373489637 | Missing |
T |
|
|
| chr19:41007013 | rs36079186 | Missing |
T |
|
|
| chr19:41009313 | Missing |
A |
|
||
| chr19:41009350 | rs45482602 | Missing |
C |
|
|
| chr19:41009358 | rs2279343 | Missing |
A |
|
|
| chr19:41010006 | rs139029625 | Missing |
G |
|
|
| chr19:41010088 | rs34698757 | Missing |
C |
|
|
| chr19:41010108 | rs193922917 | Missing |
C |
|
|
| chr19:41012316 | rs28399499 | Missing |
T |
|
|
| chr19:41012339 | rs34826503 | Missing |
C |
|
|
| chr19:41012393 | rs754621576 | Missing |
T |
|
|
| chr19:41012394 | rs780991919 | Missing |
A |
|
|
| chr19:41012465 | rs34097093 | Missing |
C |
|
|
| chr19:41012466 | rs200458614 | Missing |
G |
|
|
| chr19:41012471 | rs201500445 | Missing |
T |
|
|
| chr19:41012478 | rs200238771 | Missing |
T |
|
|
| chr19:41012693 | rs35979566 | Missing |
T |
|
|
| chr19:41012740 | rs193922918 | Missing |
G |
|
|
| chr19:41012803 | rs35010098 | Missing |
C |
|
|
| chr19:41016652 | rs764288403 | Missing |
G |
|
|
| chr19:41016679 | rs374099483 | Missing |
G |
|
|
| chr19:41016726 | rs3211369 | Missing |
A |
|
|
| chr19:41016741 | rs117872433 | Missing |
G |
|
|
| chr19:41016778 | rs564083989 | Missing |
G |
|
|
| chr19:41016805 | Missing |
A |
|
CYP2C19 allele match data
| Allele Matched: | *2/*38 |
|---|---|
| Phasing Status: |
Unphased It reports the genotype(s) that receive the highest score during the matcher process. In case of unphased data, additional genotypes might be possible and cannot be ruled out. |
| Alleles Not Considered: |
The following alleles are not considered due to 32 missing positions of the total 34 positions: *16, *30, *34 Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr10:94781859 | rs4244285 | G/A | G |
|
|
| chr10:94842866 | rs3758581 | A/G | A |
|
|
| chr10:94761900 | rs12248560 | Missing |
C |
|
|
| chr10:94762706 | rs28399504 | Missing |
A |
|
|
| chr10:94762712 | rs367543002 | Missing |
C |
|
|
| chr10:94762715 | rs367543003 | Missing |
T |
|
|
| chr10:94762755 | rs55752064 | Missing |
T |
|
|
| chr10:94762760 | rs17882687 | Missing |
A |
|
|
| chr10:94762788 | rs1564656981 | Missing |
A |
|
|
| chr10:94762856 | rs1564657013 | Missing |
A |
|
|
| chr10:94775106 | rs145328984 | Missing |
C |
|
|
| chr10:94775121 | rs1564660997 | Missing |
C |
|
|
| chr10:94775160 | rs118203756 | Missing |
G |
|
|
| chr10:94775185 | rs1288601658 | Missing |
A |
|
|
| chr10:94775367 | rs12769205 | Missing |
A |
|
|
| chr10:94775416 | rs41291556 | Missing |
T |
|
|
| chr10:94775423 | rs17885179 | Missing |
A |
|
|
| chr10:94775453 | rs72552267 | Missing |
G |
|
|
| chr10:94775489 | rs17884712 | Missing |
G |
|
|
| chr10:94775507 | rs58973490 | Missing |
G |
|
|
| chr10:94780574 | rs140278421 | Missing |
G |
|
|
| chr10:94780579 | rs370803989 | Missing |
G |
|
|
| chr10:94780653 | rs4986893 | Missing |
G |
|
|
| chr10:94781858 | rs6413438 | Missing |
C |
|
|
| chr10:94781944 | rs375781227 | Missing |
G |
|
|
| chr10:94781999 | rs72558186 | Missing |
T |
|
|
| chr10:94842861 | rs138142612 | Missing |
G |
|
|
| chr10:94842879 | rs118203757 | Missing |
G |
|
|
| chr10:94842995 | rs113934938 | Missing |
G |
|
|
| chr10:94849995 | rs17879685 | Missing |
C |
|
|
| chr10:94852738 | rs56337013 | Missing |
C |
|
|
| chr10:94852765 | rs192154563 | Missing |
C |
|
|
| chr10:94852785 | rs118203759 | Missing |
C |
|
|
| chr10:94852914 | rs55640102 | Missing |
A |
|
CYP2C9 allele match data
| Alleles Matched: |
|
|---|---|
| Phasing Status: |
Unphased It reports the genotype(s) that receive the highest score during the matcher process. In case of unphased data, additional genotypes might be possible and cannot be ruled out. |
| Alleles Not Considered: |
The following alleles are not considered due to 79 missing positions of the total 80 positions: *2, *4, *5, *6, *7, *8, *9, *10, *11, *12, *13, *14, *15, *16, *17, *19, *20, *21, *22, *23, *24, *25, *26, *27, *28, *29, *30, *31, *32, *33, *34, *35, *36, *37, *38, *39, *40, *41, *42, *43, *44, *45, *46, *47, *48, *49, *50, *51, *52, *53, *54, *55, *56, *57, *58, *59, *60, *61, *62, *63, *64, *65, *66, *67, *69, *70, *71, *72, *73, *74, *75, *76, *77, *78, *79, *80, *81, *82, *83, *84, *85 Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr10:94981296 | rs1057910 | A/C | A |
|
|
| chr10:94938683 | rs114071557 | Missing |
A |
|
|
| chr10:94938719 | Missing |
T |
|
||
| chr10:94938737 | rs67807361 | Missing |
C |
|
|
| chr10:94938771 | rs142240658 | Missing |
C |
|
|
| chr10:94938788 | Missing |
C |
|
||
| chr10:94938800 | rs1364419386 | Missing |
G |
|
|
| chr10:94938803 | rs2031308986 | Missing |
A |
|
|
| chr10:94938828 | rs564813580 | Missing |
A |
|
|
| chr10:94941897 | rs371055887 | Missing |
G |
|
|
| chr10:94941915 | Missing |
G |
|
||
| chr10:94941958 | rs72558187 | Missing |
T |
|
|
| chr10:94941975 | Missing |
G |
|
||
| chr10:94941976 | Missing |
G |
|
||
| chr10:94941982 | rs762239445 | Missing |
G |
|
|
| chr10:94942018 | Missing |
T |
|
||
| chr10:94942205 | rs1304490498 | Missing |
CAATGGAAA GA |
|
|
| chr10:94942216 | rs774607211 | Missing |
A |
|
|
| chr10:94942230 | rs767576260 | Missing |
C |
|
|
| chr10:94942231 | rs12414460 | Missing |
G |
|
|
| chr10:94942233 | rs375805362 | Missing |
C |
|
|
| chr10:94942234 | rs72558189 | Missing |
G |
|
|
| chr10:94942243 | rs1375956433 | Missing |
T |
|
|
| chr10:94942249 | rs200965026 | Missing |
C |
|
|
| chr10:94942254 | rs199523631 | Missing |
C |
|
|
| chr10:94942255 | rs200183364 | Missing |
G |
|
|
| chr10:94942290 | rs1799853 | Missing |
C |
|
|
| chr10:94942291 | rs141489852 | Missing |
G |
|
|
| chr10:94942305 | rs754487195 | Missing |
G |
|
|
| chr10:94942306 | rs1289704600 | Missing |
C |
|
|
| chr10:94942308 | rs17847037 | Missing |
C |
|
|
| chr10:94942309 | rs7900194 | Missing |
G |
|
|
| chr10:94947782 | rs72558190 | Missing |
C |
|
|
| chr10:94947785 | rs774550549 | Missing |
C |
|
|
| chr10:94947869 | Missing |
A |
|
||
| chr10:94947907 | Missing |
A |
|
||
| chr10:94947917 | rs1326630788 | Missing |
T |
|
|
| chr10:94947938 | rs2031531005 | Missing |
A |
|
|
| chr10:94947939 | rs370100007 | Missing |
G |
|
|
| chr10:94949129 | Missing |
A |
|
||
| chr10:94949144 | Missing |
C |
|
||
| chr10:94949145 | rs772782449 | Missing |
C |
|
|
| chr10:94949161 | Missing |
AT |
|
||
| chr10:94949217 | rs2256871 | Missing |
A |
|
|
| chr10:94949280 | rs9332130 | Missing |
A |
|
|
| chr10:94949281 | rs9332131 | Missing |
GA |
|
|
| chr10:94972119 | rs182132442 | Missing |
C |
|
|
| chr10:94972123 | Missing |
C |
|
||
| chr10:94972134 | Missing |
A |
|
||
| chr10:94972179 | rs72558192 | Missing |
A |
|
|
| chr10:94972180 | rs988617574 | Missing |
C |
|
|
| chr10:94972183 | Missing |
A |
|
||
| chr10:94972233 | rs1237225311 | Missing |
C |
|
|
| chr10:94981199 | Missing |
G |
|
||
| chr10:94981201 | rs57505750 | Missing |
T |
|
|
| chr10:94981224 | rs28371685 | Missing |
C |
|
|
| chr10:94981225 | rs367826293 | Missing |
G |
|
|
| chr10:94981230 | rs1274535931 | Missing |
C |
|
|
| chr10:94981250 | rs750820937 | Missing |
C |
|
|
| chr10:94981258 | rs1297714792 | Missing |
C |
|
|
| chr10:94981281 | rs749060448 | Missing |
G |
|
|
| chr10:94981297 | rs56165452 | Missing |
T |
|
|
| chr10:94981301 | rs28371686 | Missing |
C |
|
|
| chr10:94981302 | rs1250577724 | Missing |
C |
|
|
| chr10:94981305 | rs578144976 | Missing |
C |
|
|
| chr10:94981365 | Missing |
C |
|
||
| chr10:94981371 | rs542577750 | Missing |
G |
|
|
| chr10:94986042 | rs764211126 | Missing |
A |
|
|
| chr10:94986073 | rs72558193 | Missing |
A |
|
|
| chr10:94986136 | rs1254213342 | Missing |
A |
|
|
| chr10:94986174 | rs1441296358 | Missing |
G |
|
|
| chr10:94988852 | rs776908257 | Missing |
C |
|
|
| chr10:94988855 | Missing |
A |
|
||
| chr10:94988880 | Missing |
G |
|
||
| chr10:94988917 | rs769942899 | Missing |
G |
|
|
| chr10:94988925 | rs202201137 | Missing |
A |
|
|
| chr10:94988955 | rs767284820 | Missing |
T |
|
|
| chr10:94988984 | rs781583846 | Missing |
G |
|
|
| chr10:94989020 | rs9332239 | Missing |
C |
|
|
| chr10:94989023 | rs868182778 | Missing |
G |
|
Other Positions of Interest
| Position in VCF | RSID | Call in VCF |
|---|---|---|
| chr10:94645745 | rs12777823 | missing |
DPYD allele match data
| Variants Matched: |
|
|---|---|
| Phasing Status: |
Unphased |
| Alleles Not Considered: |
The following alleles are not considered due to 81 missing positions of the total 83 positions: c.46C>G, c.61C>T, c.62G>A, c.295_298delTCAT (*7), c.313G>A, c.343A>G, c.451A>G, c.498G>A, c.525G>A, c.557A>G, c.601A>C, c.632A>G, c.703C>T (*8), c.775A>G, c.868A>G, c.929T>C, c.934C>T, c.967G>A, c.1003G>T (*11), c.1024G>A, c.1057C>T, c.1108A>G, c.1129-5923C>G, c.1129-5923C>G, c.1236G>A (HapB3), c.1156G>T (*12), c.1180C>T, c.1181G>T, c.1218G>A, c.1260T>A, c.1278G>T, c.1294G>A, c.1314T>G, c.1349C>T, c.1358C>G, c.1371C>T, c.1403C>A, c.1475C>T, c.1484A>G, c.1519G>A, c.1543G>A, c.1577C>G, c.1601G>A (*4), c.1615G>A, c.1627A>G (*5), c.1679T>G (*13), c.1682G>T, c.1774C>T, c.1775G>A, c.1777G>A, c.1796T>C, c.1896T>C, c.1898delC (*3), c.1905+1G>A (*2A), c.1905C>G, c.1906A>C, c.1990G>T, c.2021G>A, c.2161G>A, c.2186C>T, c.2194G>A (*6), c.2195T>G, c.2279C>T, c.2303C>A, c.2336C>A, c.2482G>A, c.2582A>G, c.2623A>C, c.2639G>T, c.2656C>T, c.2657G>A (*9B), c.2846A>T, c.2872A>G, c.2915A>G, c.2921A>T, c.2933A>G, c.2977C>T, c.2978T>G, c.2983G>T (*10), c.3049G>A, c.3061G>C, c.3067C>A Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr1:97699535 | rs2297595 | T/C | T |
|
|
| chr1:97883329 | rs1801265 | A/G | A |
|
|
| chr1:97078987 | rs114096998 | Missing |
G |
|
|
| chr1:97078993 | rs148799944 | Missing |
C |
|
|
| chr1:97079005 | rs140114515 | Missing |
C |
|
|
| chr1:97079071 | rs1801268 | Missing |
C |
|
|
| chr1:97079076 | rs139459586 | Missing |
A |
|
|
| chr1:97079077 | rs202144771 | Missing |
G |
|
|
| chr1:97079121 | rs72547601 | Missing |
T |
|
|
| chr1:97079133 | rs72547602 | Missing |
T |
|
|
| chr1:97079139 | rs145529148 | Missing |
T |
|
|
| chr1:97082365 | rs141044036 | Missing |
T |
|
|
| chr1:97082391 | rs67376798 | Missing |
T |
|
|
| chr1:97098598 | rs1801267 | Missing |
C |
|
|
| chr1:97098599 | rs147545709 | Missing |
G |
|
|
| chr1:97098616 | rs55674432 | Missing |
C |
|
|
| chr1:97098632 | rs201035051 | Missing |
T |
|
|
| chr1:97193109 | rs60139309 | Missing |
T |
|
|
| chr1:97193209 | rs200687447 | Missing |
C |
|
|
| chr1:97234958 | rs199634007 | Missing |
G |
|
|
| chr1:97234991 | rs56005131 | Missing |
G |
|
|
| chr1:97305279 | rs112766203 | Missing |
G |
|
|
| chr1:97305363 | rs60511679 | Missing |
A |
|
|
| chr1:97305364 | rs1801160 | Missing |
C |
|
|
| chr1:97305372 | rs146529561 | Missing |
G |
|
|
| chr1:97306195 | rs145548112 | Missing |
C |
|
|
| chr1:97373598 | rs137999090 | Missing |
C |
|
|
| chr1:97373629 | rs138545885 | Missing |
C |
|
|
| chr1:97382461 | rs55971861 | Missing |
T |
|
|
| chr1:97450058 | rs3918290 | Missing |
C |
|
|
| chr1:97450059 | rs3918289 | Missing |
G |
|
|
| chr1:97450065 | rs72549303 | Missing |
TG |
|
|
| chr1:97450068 | rs17376848 | Missing |
A |
|
|
| chr1:97450168 | rs147601618 | Missing |
A |
|
|
| chr1:97450187 | rs145773863 | Missing |
C |
|
|
| chr1:97450189 | rs138616379 | Missing |
C |
|
|
| chr1:97450190 | rs59086055 | Missing |
G |
|
|
| chr1:97515784 | rs201615754 | Missing |
C |
|
|
| chr1:97515787 | rs55886062 | Missing |
A |
|
|
| chr1:97515839 | rs1801159 | Missing |
T |
|
|
| chr1:97515851 | rs142619737 | Missing |
C |
|
|
| chr1:97515865 | rs1801158 | Missing |
C |
|
|
| chr1:97515889 | rs190951787 | Missing |
G |
|
|
| chr1:97515923 | rs148994843 | Missing |
C |
|
|
| chr1:97549565 | rs138391898 | Missing |
C |
|
|
| chr1:97549600 | rs111858276 | Missing |
T |
|
|
| chr1:97549609 | rs72549304 | Missing |
G |
|
|
| chr1:97549681 | rs199549923 | Missing |
G |
|
|
| chr1:97549713 | rs57918000 | Missing |
G |
|
|
| chr1:97549726 | rs144395748 | Missing |
G |
|
|
| chr1:97549735 | rs72975710 | Missing |
G |
|
|
| chr1:97573785 | rs186169810 | Missing |
A |
|
|
| chr1:97573805 | rs142512579 | Missing |
C |
|
|
| chr1:97573821 | rs764666241 | Missing |
C |
|
|
| chr1:97573839 | rs200064537 | Missing |
A |
|
|
| chr1:97573863 | rs56038477 | Missing |
C |
|
|
| chr1:97573881 | rs61622928 | Missing |
C |
|
|
| chr1:97573918 | rs143815742 | Missing |
C |
|
|
| chr1:97573919 | rs140602333 | Missing |
G |
|
|
| chr1:97573943 | rs78060119 | Missing |
C |
|
|
| chr1:97579893 | rs75017182 | Missing |
G |
|
|
| chr1:97593238 | rs72549305 | Missing |
T |
|
|
| chr1:97593289 | rs143154602 | Missing |
G |
|
|
| chr1:97593322 | rs183385770 | Missing |
C |
|
|
| chr1:97593343 | rs72549306 | Missing |
C |
|
|
| chr1:97593379 | rs201018345 | Missing |
C |
|
|
| chr1:97595083 | rs145112791 | Missing |
G |
|
|
| chr1:97595088 | rs150437414 | Missing |
A |
|
|
| chr1:97595149 | rs146356975 | Missing |
T |
|
|
| chr1:97679170 | rs45589337 | Missing |
T |
|
|
| chr1:97691776 | rs1801266 | Missing |
G |
|
|
| chr1:97699399 | rs72549307 | Missing |
T |
|
|
| chr1:97699430 | rs72549308 | Missing |
T |
|
|
| chr1:97699474 | rs115232898 | Missing |
T |
|
|
| chr1:97699506 | rs6670886 | Missing |
C |
|
|
| chr1:97699533 | rs139834141 | Missing |
C |
|
|
| chr1:97721542 | rs200562975 | Missing |
T |
|
|
| chr1:97721650 | rs141462178 | Missing |
T |
|
|
| chr1:97740400 | rs150385342 | Missing |
C |
|
|
| chr1:97740410 | rs72549309 | Missing |
GATGA |
|
|
| chr1:97883352 | rs80081766 | Missing |
C |
|
|
| chr1:97883353 | rs72549310 | Missing |
G |
|
|
| chr1:97883368 | rs150036960 | Missing |
G |
|
SLCO1B1 allele match data
| Allele Matched: | *1/*20 |
|---|---|
| Phasing Status: |
Unphased It reports the genotype(s) that receive the highest score during the matcher process. In case of unphased data, additional genotypes might be possible and cannot be ruled out. |
| Alleles Not Considered: |
The following alleles are not considered due to 29 missing positions of the total 31 positions: *2, *3, *4, *5, *6, *7, *8, *9, *10, *11, *12, *13, *16, *23, *26, *34, *36, *38, *41, *45 Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
In case no genotype can be determined, recommendations are based on the rs4149056 genotype alone as per guideline. The minor C allele at rs4149056 defines SLCO1B1*5.
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr12:21176804 | rs2306283 | A/G | A |
|
|
| chr12:21239042 | rs34671512 | A/C | A |
|
|
| chr12:21172734 | rs139257324 | Missing |
C |
|
|
| chr12:21172776 | rs373327528 | Missing |
G |
|
|
| chr12:21172782 | rs56101265 | Missing |
T |
|
|
| chr12:21174595 | rs56061388 | Missing |
T |
|
|
| chr12:21176868 | rs2306282 | Missing |
A |
|
|
| chr12:21176871 | Missing |
G |
|
||
| chr12:21176879 | rs11045819 | Missing |
C |
|
|
| chr12:21176883 | rs72559745 | Missing |
A |
|
|
| chr12:21176898 | rs77271279 | Missing |
G |
|
|
| chr12:21178612 | rs141467543 | Missing |
A |
|
|
| chr12:21178615 | rs4149056 | Missing |
T |
|
|
| chr12:21178957 | rs79135870 | Missing |
A |
|
|
| chr12:21196951 | rs11045852 | Missing |
A |
|
|
| chr12:21196975 | rs183501729 | Missing |
C |
|
|
| chr12:21196976 | rs11045853 | Missing |
G |
|
|
| chr12:21200544 | rs72559747 | Missing |
C |
|
|
| chr12:21200595 | rs55901008 | Missing |
T |
|
|
| chr12:21202553 | rs1228465562 | Missing |
T |
|
|
| chr12:21202555 | rs59113707 | Missing |
C |
|
|
| chr12:21202649 | rs56387224 | Missing |
A |
|
|
| chr12:21202664 | rs142965323 | Missing |
G |
|
|
| chr12:21205921 | rs72559748 | Missing |
A |
|
|
| chr12:21205999 | rs59502379 | Missing |
G |
|
|
| chr12:21206031 | rs74064213 | Missing |
A |
|
|
| chr12:21222355 | rs71581941 | Missing |
C |
|
|
| chr12:21239077 | rs56199088 | Missing |
A |
|
|
| chr12:21239113 | rs55737008 | Missing |
A |
|
|
| chr12:21239145 | rs200995543 | Missing |
C |
|
|
| chr12:21239158 | rs140790673 | Missing |
C |
|
TPMT allele match data
| Allele Matched: | *1/*3A |
|---|---|
| Phasing Status: |
Unphased It reports the genotype(s) that receive the highest score during the matcher process. In case of unphased data, additional genotypes might be possible and cannot be ruled out. |
| Alleles Not Considered: |
The following alleles are not considered due to 41 missing positions of the total 43 positions: *2, *4, *5, *6, *7, *8, *9, *10, *11, *12, *13, *14, *15, *16, *17, *18, *19, *20, *21, *22, *23, *24, *25, *26, *27, *28, *29, *30, *31, *32, *33, *34, *35, *36, *37, *38, *39, *40, *42, *43, *44 Carriage of these alleles might result in a different phenotype and different guideline recommendations. |
Calls at Positions
| Position in VCF | RSID | Call in VCF | Reference | Related Alleles and Function | Warnings |
|---|---|---|---|---|---|
| chr6:18130687 | rs1142345 | T/C | T |
|
|
| chr6:18138997 | rs1800460 | C/T | C |
|
|
| chr6:18130694 | rs150900439 | Missing |
T |
|
|
| chr6:18130725 | rs72552736 | Missing |
A |
|
|
| chr6:18130729 | rs139392616 | Missing |
C |
|
|
| chr6:18130758 | rs398122996 | Missing |
A |
|
|
| chr6:18130762 | rs56161402 | Missing |
C |
|
|
| chr6:18130772 | rs377085266 | Missing |
A |
|
|
| chr6:18130781 | rs1800584 | Missing |
C |
|
|
| chr6:18132136 | rs72556347 | Missing |
A |
|
|
| chr6:18132147 | rs79901429 | Missing |
A |
|
|
| chr6:18132163 | Missing |
C |
|
||
| chr6:18133845 | rs75543815 | Missing |
T |
|
|
| chr6:18133847 | rs6921269 | Missing |
C |
|
|
| chr6:18133870 | rs772832951 | Missing |
A |
|
|
| chr6:18133884 | rs74423290 | Missing |
G |
|
|
| chr6:18133887 | rs201695576 | Missing |
T |
|
|
| chr6:18133890 | rs9333570 | Missing |
C |
|
|
| chr6:18138969 | rs144041067 | Missing |
C |
|
|
| chr6:18138970 | rs112339338 | Missing |
G |
|
|
| chr6:18139027 | rs72552737 | Missing |
C |
|
|
| chr6:18139689 | rs72552738 | Missing |
C |
|
|
| chr6:18139710 | rs200220210 | Missing |
G |
|
|
| chr6:18143597 | Missing |
T |
|
||
| chr6:18143606 | rs151149760 | Missing |
T |
|
|
| chr6:18143613 | Missing |
C |
|
||
| chr6:18143622 | rs115106679 | Missing |
C |
|
|
| chr6:18143643 | Missing |
A |
|
||
| chr6:18143700 | rs753545734 | Missing |
C |
|
|
| chr6:18143718 | rs111901354 | Missing |
G |
|
|
| chr6:18143724 | rs1800462 | Missing |
C |
|
|
| chr6:18143728 | rs1256618794 | Missing |
C |
|
|
| chr6:18147838 | rs281874771 | Missing |
G |
|
|
| chr6:18147845 | rs777686348 | Missing |
C |
|
|
| chr6:18147851 | rs200591577 | Missing |
G |
|
|
| chr6:18147856 | Missing |
A |
|
||
| chr6:18147910 | rs72552740 | Missing |
A |
|
|
| chr6:18149004 | Missing |
G |
|
||
| chr6:18149022 | rs750424422 | Missing |
C |
|
|
| chr6:18149032 | rs759836180 | Missing |
C |
|
|
| chr6:18149045 | rs72552742 | Missing |
T |
|
|
| chr6:18149126 | rs267607275 | Missing |
A |
|
|
| chr6:18149127 | rs9333569 | Missing |
T |
|
Disclaimers and Other Information
Liability: This report assumes no responsibility for any injury to person or damage to persons or property arising out of, or related to any use of this report, or for any errors or omissions. The user recognizes that this report is a research tool and that they are using this report at their own risk.
A. Allele and Genotype Determination
This report uses gene allele definitions included in the CPIC database, with exceptions "CYP3A4, DPYD, G6PD, NAT2, SLCO1B1, RYR1". For allele definitions and the positions used in this report, see the gene definition tables.
Genes with DPWG recommendations that are not included in CPIC are discussed in Section C.
This report results are dependent on the supplied VCF calls for the queried positions. For technical information about input formatting and requirements, please refer to the relevant documentation. This report does not assume any reference calls for positions missing from the submitted VCF file; all missing queried positions are not considered in the allele determination process. Missing positions might alter the assigned genotype and subsequent phenotype prediction and CPIC recommendation. If the supplied VCF file has missing positions, those positions will be noted in Section III: Allele Matching Details for each gene of this report. For the most reliable allele determination, reference calls as well as variant calls in the VCF file for every queried position must be provided by the user. If an allele that includes a missing position is defined by an additional position(s) for which calls are provided, the allele will be considered in the matching process based on the available information. This might lead to the output of multiple possible genotypes that received the same highest matching score. In addition, alternate calls with a lower score is also possible. For instructions on getting this report to output all possible matching genotypes, consult the relevant documentation.
For cytochrome P450 genes, TPMT, NUDT15, UGT1A1, and SLCO1B1, the *1 allele is defined by the absence of variation specified in the gene definition tables. This allele cannot be identified by variants; rather, *1 is assigned by default when no variation for the queried positions is reported in the submitted VCF file. The same is true for all other genes with multiple variant positions in the definition table (CACNA1S, CFTR, DPYD, RYR1): the reference sequence is the default result when variants are not reported in the VCF file. It is always possible un-interrogated variation can occur which could potentially affect allele function, but because it is undetected, the assignment would be defaulted to a *1 (or reference) allele and normal function.
For all genes, variation reported in the VCF file but NOT included in the gene definition table will not be considered during allele assignment. There is a possibility that any such variation results in a reduced or no activity allele which could lead to inaccurate phenotype and CPIC recommendation.
Nucleotide base calls are displayed on the positive chromosomal strand regardless of the gene strand; further information is provided under Gene-specific warnings in Section III: Allele Matching Details.
Structural variation star alleles that cannot be detected using VCF file data:
- CYP2B7-CYP2B6 hybrids: CYP2B6*29, CYP2B6*30
- Partial and whole gene deletions: CYP2C19*36, CYP2C19*37, CYP4F2*16, SLCO1B1*48, SLCO1B1*49
This report matches variants to genotypes assuming unphased data (unless phased data is provided in the VCF file and noted as such, see the relevant documentation for details). The assumption is that defined alleles exist in trans configuration, i.e. on opposite chromosomes, with exceptions noted in Section III: Allele Matching Details under "Gene-specific warnings." However, in cases where an allele is defined by a combination of two or more variants, where each variant alone also defines an allele, the match is based on the longer allele. For example, TPMT*3B is defined by one SNP, *3C is defined by another SNP, and *3A is defined by the combination of those two SNPs. In the case of unphased data that is heterozygous for both SNPs, the *1/*3A genotype is returned though the possibility of *3B/*3C cannot be ruled out.
Below cases are summarized for which two calls with different scores are possible when provided unphased data and heterozygous calls for the variants that define the two alleles. The genotype with the higher score (longer allele) will be used to determine allele functionality, phenotype, and recommendation but the genotype with the lower score cannot be ruled out.
Table 1: Cases for which there is an overlap in the allele definitions.
| Gene | Genotype (Higher Score) | Phenotype | Genotype (Lower Score) | Phenotype |
|---|---|---|---|---|
| UGT1A1 | *1/*80+*28 | Intermediate | *28/*80 | Indeterminate |
| UGT1A1 | *1/*80+*37 | Intermediate | *37/*80 | Indeterminate |
| TPMT | *1/*3A | Intermediate | *3B/*3C | Poor |
| NUDT15 | *1/*2 | Intermediate | *3/*6 | Possible Intermediate |
| CYP2C9 | *1/*71 | N/A | *10/*22 | Indeterminate |
| CYP2B6 | *1/*36 | Intermediate | *6/*22 | Intermediate |
| CYP2B6 | *1/*34 | Intermediate | *33/*36 | Indeterminate |
| CYP2B6 | *1/*6 | Intermediate | *4/*9 | Intermediate |
| CYP2B6 | *1/*7 | Intermediate | *5/*6 | Intermediate |
| CYP2B6 | *1/*13 | Intermediate | *6/*8 | Intermediate |
| SLCO1B1 | *1/*46 | Decreased function | *15/*45 | Possible Decreased Function |
| SLCO1B1 | *1/*20 | Normal Function | *19/*37 | Indeterminate |
| SLCO1B1 | *1/*12 | Indeterminate | *2/*10 | Indeterminate |
| SLCO1B1 | *1/*13 | Indeterminate | *3/*11 | Indeterminate |
| SLCO1B1 | *1/*14 | Normal Function | *4/*37 | Indeterminate |
| SLCO1B1 | *1/*15 | Decreased function | *5/*37 | Decreased function |
| SLCO1B1 | *1/*25 | Indeterminate | *4/*28 | Indeterminate |
| SLCO1B1 | *1/*31 | Decreased function | *9/*37 | Decreased Function |
| SLCO1B1 | *1/*32 | Indeterminate | *4/*24 | Indeterminate |
| SLCO1B1 | *1/*40 | Indeterminate | *5/*19 | Possible Decreased Function |
| SLCO1B1 | *1/*43 | Indeterminate | *4/*44 | Indeterminate |
| CYP4F2 | *1/*4 | N/A | *2/*3 | N/A |
| CYP3A4 | *1/*37 | N/A | *3/*22 | N/A |
| CYP3A4 | *1/*38 | N/A | *3/*11 | N/A |
| G6PD | A- 202A_376G/B (reference) | Variable | A/Asahi | Variable |
| G6PD | B (reference)/Mt Sinai | Variable | A/Guadalajara | Variable |
| G6PD | B (reference)/Santa Maria | Variable | A/Malaga | Variable |
| G6PD | Ananindeua/B (reference) | Variable | A/Viangchan, Jammu | Variable |
| G6PD | B (reference)/Hechi | Variable | Asahi/Viangchan, Jammu | Deficient |
| G6PD | B (reference)/Hermoupolis | Variable | Cassano/Union,Maewo, Chinese-2, Kalo | Deficient |
Table 2: Cases for which there is an overlap in the allele definitions because the definition of the non-*1 allele in the genotype with the higher score allows for reference or variant at the position that defines the first allele listed in the genotype with the lower score. Both genotypes cannot be ruled out with unphased data if the position that overlaps between the respective alleles is heterozygous (0/1) in addition to heterozygous calls for the other variants that define the non-*1 allele in the genotype with the higher score.
| Gene | Genotype (Higher Score) | Phenotype | Genotype (Lower Score) | Phenotype |
|---|---|---|---|---|
| CYP2C19 | *1/*4 | Intermediate | *17/*4 | Intermediate |
| CYP2C19 | *1/*2 | Intermediate | *11/*2 | Intermediate |
| CYP2C19 | *1/*35 | Intermediate | *15/*35 | Intermediate |
| CYP2B6 | *1/*18 | Intermediate | *4/*18 | Indeterminate |
B. CPIC Allele Function, Phenotype and Recommendation
All content is sourced from the CPIC database.
C. DPWG Allele Function, Phenotype and Recommendation
PharmGKB annotates PGx-based drug dosing guidelines published by the Royal Dutch Association for the Advancement of Pharmacy - Pharmacogenetics Working Group (DPWG). PharmGKB curates allele function assignments and phenotype mappings from the DPWG to provide genotype specific DPWG guideline recommendations. Where possible, PharmGKB maps DPWG terms to CPIC terms, as outlined on PharmGKB.
CYP3A4 is currently not part of a CPIC guideline. Since the DPWG CYP3A4 documentation includes limit variant notations for the included alleles (only *16, *20, and *22 are specified). This report relies on PharmVar CYP3A4 allele definitions. However, the CYP3A4*16, *20 and *22 definitions are the same in both sources.
The CPIC UGT1A1 allele definition file includes *6, *27, *28, *36, *37, and *80. Since the DPWG UGT1A1 document does not include allele definitions besides for the UGT1A1 TA box promoter polymorphism, this report only includes the UGT1A1 positions from the CPIC UGT1A1 allele definition file. Other UGT1A1 alleles can be supplied as outside calls but not be determined from the VCF file by the Named Allele Matcher.
D. FDA drug-label and Table of Pharmacogenetic Associations recommendations
This report includes recommendations from PharmGKB-annotated FDA drug labels and the FDA Table of Pharmacogenetic Associations. It only contains FDA information for genes with CPIC or DPWG guidelines because the FDA does not offer any genotype-to-phenotype mapping information. This report uses CPIC genotype-to-phenotype mappings when they exist, and DPWG genotype-to-phenotype mappings when no CPIC mappings exist, to determine the phenotypes to use with FDA label annotations and Table of Pharmacogenetic Associations entries. Results presented for FDA Table of Pharmacogenetic Associations use wording and “Affected Subgroups” taken directly from the Table. Results presented from PharmGKB-annotated drug labels present wording from the specific label that was curated. In many cases, multiple FDA labels may exist for a particular medication. Typically, PharmGKB annotates the label linked to from the FDA Table of Pharmacogenomic Biomarkers in Drug Labeling but in some cases a different label may be annotated. Follow the “FDA Label Annotation” link in section II of the report to access the annotated label and more information.
E. Source Tags in Section II
Part of PharmGKB’s annotations of guidelines, drug labels and Table of Pharmacogenetic Associations is the assignment of labels that are meant to provide a high-level indication of the provided action. If recommendations or FDA Table wording exists, yellow boxes display if the guidance/wording is regarding (1) a dosing change, (2) recommending an alternate drug be used, or (3) other guidance. These boxes are included in the Source column in Section II of the report. More detailed information about what the yellow boxes mean is available on PharmGKB.
F. Exceptions to the CPIC Guideline Gene List
This report does not determine CYP2D6, MT-RNR1, HLA-A, or HLA-B genotypes from the VCF file, but genotypes for CYP2D6, MT-RNR1, HLA-A, or HLA-B can be provided to this report from an outside source and the corresponding phenotype prescribing recommendations will be included in the generated report. For the required format of the outside calls refer to the outside calls documentation.
CPIC has assigned function to the following CYP2D6 CNV alleles: *1x2, *1x≥3, *2x2, *2x≥3, *3x2, *4x2, *4x≥3, *6x2, *9x2, *10x2, *17x2, *29x2, *35x2, *36x2, *41x2, *41x3, *43x2, *45x2, *146x2. These alleles are part of the CPIC diplotype to phenotype translation and can be connected to recommendations. Other CNV notations from outside calls need to be mapped accordingly.
G. CPIC Guideline Disclaimers and Caveats
A version of the following quoted disclaimer is part of each CPIC guideline and applies to the CPIC recommendations as used in this report. For the full description of potential benefits and risks, additional considerations (general and specific to gene-drug pairs), limitations, information about respective gene nomenclature systems, potential drug-drug interactions and clinical factors to consider, please see individual CPIC guidelines at (cpicpgx.org).
"CPIC guidelines reflect expert consensus based on clinical evidence and peer-reviewed literature available at the time they are written and are intended only to assist clinicians in decision-making and to identify questions for further research. New evidence may have emerged since the time a guideline was submitted for publication. Guidelines are limited in scope and are not applicable to interventions or diseases not specifically identified. Guidelines do not account for all individual variations among patients and cannot be considered inclusive of all proper methods of care or exclusive of other treatments. It remains the responsibility of the health-care provider to determine the best course of treatment for a patient. Adherence to any guidelines is voluntary, with the ultimate determination regarding its application to be made solely by the clinician and the patient. CPIC assumes no responsibility for any injury to persons or damage to persons or property arising out of or related to any use of CPIC's guidelines, or for any errors or omissions." (PMID: 27997040)
"Caveats: appropriate use and/or potential misuse of genetic tests. The application of genotype-based dosing is most appropriate when initiating therapy with a tricyclic. Obtaining a pharmacogenetic test after months of drug therapy may be less helpful in some instances, as the drug dose may have already been adjusted based on plasma concentrations, response, or side effects. Similar to all diagnostic tests, genetic tests are one of several pieces of clinical information that should be considered before initiating drug therapy." (PMID: 27997040)
CPIC guidelines reflect the alleles/genotypes known and considered by the guideline authors for inclusion by the time of publication, however they may be updated online at cpicpgx.org and in the CPIC database in between publications. Additional alleles and/or more extensive allele definitions might exist by the representative gene nomenclatures for various genes.
CPIC is a registered service mark of the U.S. Department of Health & Human Services (HHS).
H. Disclaimers and Caveats
PharmGKB is a registered service mark of the U.S. Department of Health & Human Services (HHS).